Medicare Program Integrity and Efforts to Root Out Improper Payments, Fraud, Waste and Abuse
Medicare, the federal health insurance program for people ages 65 and older and people under 65 with long-term disabilities, covers 68 million people and represents 15% of all federal spending – nearly $1 trillion dollars in 2024. The Medicare program has more than 1.4 million providers and more than 20 different payment systems. Due to the complexity and size of the program, Medicare faces risk of improper payments and some vulnerability to fraud, waste, and abuse, though many actions have been taken over the years to reduce improper payments in the program and to root out fraud.
President Trump has established a government cost-cutting initiative known as the “Department of Government Efficiency” or DOGE, which has set about to dramatically overhaul the size and scope of federal government spending. The leader of DOGE, Elon Musk, recently claimed that “big money fraud” is happening at the Centers for Medicare & Medicaid Services (CMS) and that “the waste and fraud in entitlement spending, which is most of the federal spending, is entitlements, so that’s the big one to eliminate.”
Strengthening program integrity and tackling fraud, waste, and abuse in Medicare, as well as in other government programs, has been a priority across prior administrations. During President Obama’s administration, President Trump’s first term and during President Biden’s administration, the Department of Health and Human Services (HHS) budgets included proposals to improve program integrity, including for Medicare and Medicaid, reduce improper payments for these and other programs, and provide additional funding to combat fraud, waste, and abuse.
CMS, primarily through the Center for Program Integrity (CPI), plays a key role in efforts to promote program integrity in Medicare. In addition, the HHS Office of Inspector General (HHS OIG), often in collaboration with the Department of Justice (DOJ) and other agencies, monitors and combats fraud, waste, and abuse to improve the efficiency of Medicare by conducting audits, evaluations, and investigations, and carrying out enforcement actions, which in some instances have resulted in criminal or civil penalties. Despite the HHS Inspector General playing a key role in providing oversight of program integrity efforts for Medicare and other HHS programs, President Trump fired the HHS Inspector General and several other Inspectors General just days after taking office for his second term.
This brief explains fraud, waste, abuse, and improper payments in Medicare and describes actions to ensure Medicare program integrity.
Fraud, waste, abuse, and improper payments are often used interchangeably but have distinct meanings in the context of Medicare.
Improper payments. Improper payments are defined in law as “any payment that should not have been made or that was made in an incorrect amount, including an overpayment or underpayment, under a statutory, contractual, administrative, or other legally applicable requirement; and includes: any payment to an ineligible recipient; any payment for an ineligible good or service; any duplicate payment; any payment for a good or service not received, except for those payments where authorized by law; and any payment that does not account for credit for applicable discounts.”
Improper payments in the Medicare program, both overpayments and underpayments, can result from fraud, waste, and abuse as well as errors. For example, improper payments can be due to documentation mistakes or omissions, such as missing signatures, which may occur with otherwise appropriate claims and payments.
Improper payments often get conflated with fraud, and while they may be related, they are not the same. As the Government Accountability Office (GAO) explains on the relationship between fraud and improper payments, all fraudulent payments are considered improper, but not all improper payments are the result of fraud. Therefore, estimates of improper payments should not be considered estimates of fraud.
Fraud. According to CMS, Medicare fraud occurs when a provider knowingly submits false information to the federal government to receive Medicare payments. Medicare fraud can include knowingly billing for a higher level of complexity of services than the level that was actually provided, knowingly billing for services not provided, including falsifying records of providing such services, and knowingly ordering medically unnecessary items or services. Committing Medicare fraud is illegal and may lead to imprisonment, fines, and penalties. There are no estimates of how much Medicare specifically loses to fraud.
One recent example of Medicare fraud involved a $17 million Medicare hospice fraud committed against the federal government, in which an individual plead guilty to health care fraud, aggravated identity theft, and money laundering. In this case, the individual engaged in a scheme to operate a series of sham hospice companies and submitted fraudulent claims to Medicare for services that were not medically necessary and not provided, including for people who were not terminally ill and those who never received care from those sham hospices. Another example is a provider who was found guilty of health care fraud and other charges, who submitted over $24 million in fraudulent claims to Medicare, involving kickbacks and bribes for authorizing medically unnecessary cancer genetic lab tests, lengthy office visits that were never provided to patients, and medically unnecessary orthotic braces.
Abuse. According to CMS, abuse occurs when providers or suppliers perform actions that directly or indirectly result in unnecessary costs to the Medicare program. Abuse includes any practice that does not meet professionally recognized standards. Examples of abuse are billing for unnecessary medical services, charging excessively for services or supplies, or upcoding claims, which is when a provider uses an inaccurate billing code for a medical procedure that increases reimbursement. As CMS explains, “the difference between “fraud” and “abuse” depends on specific facts, circumstances, intent, and knowledge,” but fraudulent activity can be characterized by its intentional nature leading to some “unauthorized benefit.” Ultimately, CMS notes that providers who engage in abusive billing practices, like upcoding, or fraudulent activity, like charging for services that were not delivered, can be subject to civil and criminal penalties.
Waste. CMS defines waste as the overuse or misuse of resources that directly or indirectly result in unnecessary costs to the Medicare program. Examples of waste include conducting excessive office visits, prescribing more medications than necessary, and ordering excessive or duplicative laboratory tests. While the distinction between waste and abuse is not always clear, both result in unnecessary costs to the Medicare program.
CMS’s formal definition of waste differs from other views of waste, which may include value judgements of how the government should or should not be spending taxpayer money. As one example of this, MedPAC, an independent agency that advises Congress about Medicare payment, estimates the federal government pays insurers 20% more for Medicare Advantage enrollees than it pays for similar people in traditional Medicare, which amounts to $84 billion in additional annual spending in 2025 alone. Some might argue that this extra spending is wasteful while others might argue it adds value to the Medicare program by providing extra benefits to Medicare Advantage enrollees.
The vast majority of Medicare payments are made properly, although improper payments are an ongoing concern.
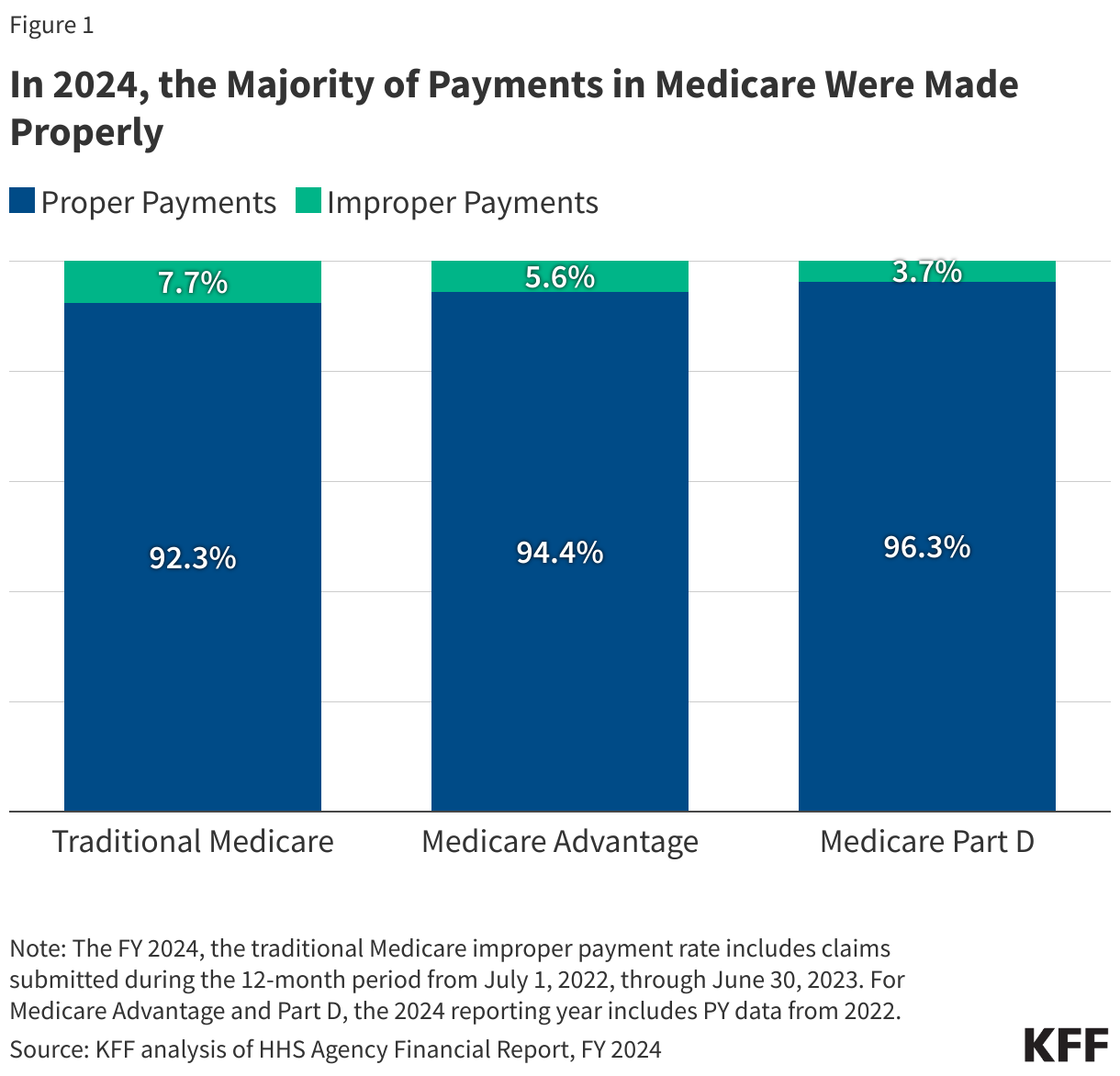
The vast majority of payments under traditional Medicare, Medicare Advantage, and Part D are made properly (Figure 1). CMS identifies, reports, and estimates improper payments for Medicare as well as other government programs, as required by the Payment Integrity Information Act of 2019 (PIIA) and as part of its integrity programs for Medicare. The improper payment rate was first measured in traditional Medicare starting in 1996 and for Medicare Advantage starting in 2008.
The Trump administration recently cited an estimate of $140 billion in improper payments made by CMS in 2024, but based on the amounts derived from each part of Medicare (as described below), improper payments for the Medicare program totaled substantially less – $54.3 billion in 2024, according to GAO. Even across all CMS programs – Medicare, Medicaid, CHIP, and the Affordable Care Act Health Insurance Exchange Advance Payments of the Premium Tax Credit (APTC) programs, the total amount of improper payments is less than the total cited by the administration – totaling $87.1 billion in 2024, according to CMS. Government-wide, 16 federal agencies across 68 programs, reported improper payments of $162 billion in 2024, a decrease of $74 billion from 2023, according to GAO. Again, estimates of improper payments described here are not the same as estimates of fraud.
CMS relies on three approaches to measure improper payments for traditional Medicare, Medicare Advantage, and Medicare Part D using different statistical methods for each:
- The Comprehensive Error Rate Testing (CERT) program measures the improper payment rate in traditional Medicare. To determine if claims were paid properly, the CERT program reviews a random sample of traditional Medicare claims – approximately 37,500 claims in 2024.
- In 2024, traditional Medicare paid an estimated 92.34% of claims properly, representing $382.02 billion in proper federal payments. The traditional Medicare improper payment rate was 7.66% (or $31.70 billion in federal payments) in 2024.
- The Medicare Part C Improper Payment Measurement (Part C IPM) measures the improper payment rate in Medicare Advantage. The program verifies that diagnosis codes submitted for payment by a Medicare Advantage organization are supported by medical record documentation based on a random sample of about 1,000 beneficiaries.
- In 2024, Medicare Advantage paid an estimated 94.39% of claims properly, representing $320.87 billion in proper federal payments. The Medicare Advantage improper payment rate was 5.61% (or $19.07 billion in federal payments) in 2024. (These estimates of improper payments in Medicare Advantage do not include estimates of higher spending in Medicare Advantage compared to traditional Medicare for similar beneficiaries as discussed above, which are often referred to as “overpayments”).
- The Medicare Part D Improper Payment Measurement (Part D IPM) measures error in payments due to inaccurate prescription drug event (PDE) records. The data is based on a randomly selected five percent sample of the Part D beneficiary population.
- In 2024, Medicare Part D paid an estimated 96.30% of claims properly, representing $92.95 billion in proper federal payments. The Medicare Part D improper payment rate was 3.70% (or $3.58 billion in federal payments) in 2024.
The rate of improper payments for traditional Medicare has decreased over time from 12.7% in FY2014 to 7.66% in FY2024. (Similar trends are not included for Medicare Advantage and Part D due to methodological changes in the calculation of the estimates over time.) While improper payment rates for traditional Medicare have generally declined, the overall amount of improper payments have increased as Medicare spending has increased over this period. Improper payments both negatively impact beneficiaries and reduce the solvency of the Medicare Hospital Insurance (Part A) Trust Fund, which is projected to be depleted in 2036.
The primary reason for improper payments differs for traditional Medicare, Medicare Part D and Medicare Advantage.
In traditional Medicare, insufficient or no documentation was the most common reason for improper payments, accounting for 68% of improper payments, similar to Medicare Part D (73%), while for Medicare Advantage, medical record discrepancies accounted for 85% of all improper payments (Figure 2).
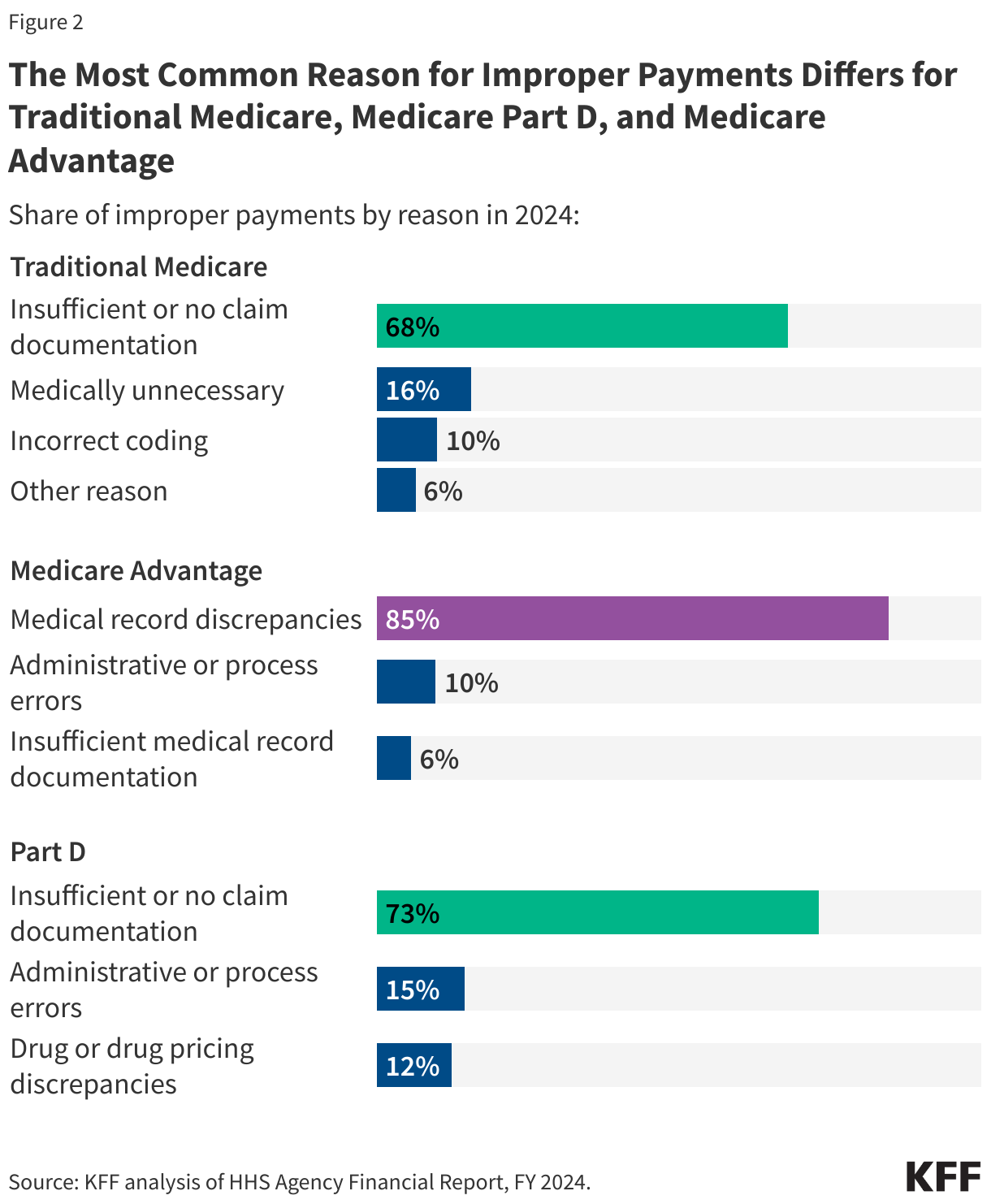
In 2024, the most common reason for improper payments in traditional Medicare was insufficient or no documentation (68%), followed by claims being medically unnecessary (16%), incorrect coding (10%), and other reasons (6%). Similarly, for Medicare Part D, insufficient or no documentation (73%) was the main reason for improper payments, followed by administrative or process errors (15%) and drug or drug pricing discrepancies (12%). The primary reason for Medicare Advantage improper payments is medical record discrepancies, accounting for 85% of all improper payments, followed by administrative or process errors (10%) and insufficient documentation (6%). According to CMS, improper payments due to medical record discrepancies result when medical record documentation submitted by a Medicare Advantage plan does not support payments received by the plan.
The differences in the main drivers of improper payments in traditional Medicare, Medicare Part D and Medicare Advantage reflect in part how improper payments are calculated – for traditional Medicare, CERT evaluates claims submitted by providers, and for Part D, the Part D IPM evaluates errors in payments for prescription drug claims, while for Medicare Advantage, the Part C IPM evaluates whether submitted diagnoses codes for which Medicare Advantage plans received payment are supported by enrollees’ medical records. Improper payments can result in either overpayments (monetary loss) or underpayments (non-monetary loss).
CMS is responsible for many program integrity activities, including conducting audits to identify and recover Medicare improper payments.
The CMS Center for Program Integrity (CPI) primarily implements the Medicare Integrity Program, which is responsible for helping to protect Medicare against fraud, waste, and abuse for various parts of the Medicare program. Program integrity activities within CMS resulted in estimated Medicare savings of $14.9 billion in FY 2023 and produced a substantial return on investment (ROI) – for every $1 spent on program integrity efforts, Medicare saved $8.30.
Among the many program integrity activities conducted by CMS to root out fraud, waste, abuse, and address improper payments in traditional Medicare and Medicare Advantage, audits are an important tool, including the Medicare Fee for Service Recovery Audit Program and the Medicare Advantage Risk Adjustment Data Validation audits.
- The Medicare Fee for Service Recovery Audit Program. The Medicare Fee for Service (FFS) Recovery Audit Program’s mission is to identify and correct Medicare improper payments made on claims of health care services provided to traditional Medicare beneficiaries and recover those improper payments. In FY 2023, Recovery Audit Contractors (RACs) identified $353 million in overpayments and recovered $273 million. Recovery audits are distinct from CERT audits in that they seek to both identify and recover improper payments, while the CERT audits provide a national estimate of improper payments in traditional Medicare.
- Medicare Advantage Risk Adjustment Data Validation (RADV) audits. Medicare Advantage RADV audits have similar objectives to the Medicare Fee for Service Recovery Audit Program and are the primary way CMS identifies and collects improper payments in Medicare Advantage. As part of RADV audits, CMS confirms that diagnoses submitted by Medicare Advantage organizations for risk adjustment are supported by enrollees’ medical records. Medicare Advantage organizations are held financially accountable when data submitted for risk adjustment purposes do not align with program rules. If Medicare Advantage organizations do not agree with the audit results, they may appeal these medical record review determinations. RADV audits, conducted by the CPI, seek to both identify and recover improper payments from Medicare Advantage plans, while Part C IPM audits provide a national estimate of improper payments in Medicare Advantage.
In 2023, the Biden Administration finalized a rule, which was proposed in 2018 during the first Trump administration, to make adjustments to the RADV program. One of the major elements of the finalized rule was the decision to extrapolate payments, which is a technique widely used in traditional Medicare and other audits, to estimate values, such as overpayments, based on a statistically random sample that would apply to the entire Medicare Advantage contract. The final rule extrapolates contract-level findings for audits starting in payment year 2018. In September 2023, Humana sued the government over its methodology and a federal judge denied dismissal of the case in June 2024, but the final outcome of the case is still pending.
The HHS OIG, DOJ, and other agencies play a major role in combatting Medicare fraud, waste, abuse and improper payments.
The HHS OIG, established through legislation in 1976, has played a major role in monitoring and combating fraud, waste and abuse to improve the efficiency of Medicare and other HHS programs, with the majority of its resources going to oversight of Medicare and Medicaid. The HHS OIG has a variety of responsibilities including conducting and supervising audits, investigations, and evaluations relating to HHS programs; identifying systemic weaknesses that give rise to opportunities for fraud and abuse and making recommendations to prevent them from reoccurring; leading and coordinating activities to prevent and detect fraud and abuse; and imposing administrative sanctions against providers of health care under Medicare and Medicaid who commit certain prohibited acts. The HHS OIG also operates a fraud hotline where it accepts tips and complaints related to potential fraud, waste, and abuse in HHS programs.
As the number of beneficiaries enrolled in Medicare Advantage has increased, the HHS OIG has focused more of its efforts on addressing the risks of fraud, waste, and abuse in Medicare Advantage and has developed a strategic plan for its oversight. One of its main priorities is ensuring that payments to Medicare Advantage plans are accurate. Similar to the RADV audits mentioned above that are conducted by CMS, the HHS OIG regularly audits Medicare Advantage organizations to review the accuracy of diagnosis codes since some diagnoses are at higher risk of being miscoded, resulting in overpayments to these organizations. For example, two of OIG’s recent audits released in December 2024, found that Medicare Advantage plans had submitted diagnosis codes that did not comply with federal requirements, resulting in millions of dollars in estimated overpayments, though both plans disputed OIG’s findings and recommendations. HHS OIG audits do not represent final determinations and CMS officials ultimately determine whether the agency will seek to recoup overpayments in these instances.
The HHS OIG has also examined the use of health risk assessments (HRAs) and chart reviews in Medicare Advantage, producing multiple reports on how these activities can increase risk scores and drive billions of dollars in additional payments to Medicare Advantage plans. As mentioned above, MedPAC estimates the federal government pays more for Medicare Advantage enrollees than it pays for similar people in traditional Medicare, at a cost of $84 billion in 2025 – $40 billion of which can be attributed to coding differences that increase payments to Medicare Advantage plans.
The HHS OIG often collaborates with the DOJ to fulfill its duties. OIG works with DOJ, under the joint direction of the Attorney General and the Secretary of Health and Human Services (HHS), to operate the Health Care Fraud and Abuse Control (HCFAC) Program, which was established in 1996 as part of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) by the Clinton administration. The Program is tasked with coordinating federal, state, and local law enforcement efforts relating to health care fraud for Medicare, Medicaid, and other health care programs, conducting investigations and audits relating to the delivery of and payment for health care, and enforcing remedies for fraud.
The DOJ and U.S. Attorneys carry out enforcement actions against those suspected of engaging in Medicare fraud, including bringing criminal and civil cases to stop ongoing fraud, deter future fraud, and recover funds wrongfully taken through fraud and false claims. In FY 2023, 476 defendants were convicted of health care fraud-related crimes, which includes but is not limited to Medicare. In its annual report on the Health Care Fraud and Abuse Control Program, the OIG highlighted significant criminal and civil investigations for Medicare and other federal health care programs including in the areas of ambulances, diagnostic testing, durable medical equipment, home health providers, hospice, and medical devices, among others.
The DOJ has also been involved in civil cases regarding Medicare Advantage insurers, often in relation to allegations of false diagnosis codes submitted to inflate Medicare payments to plans through the risk adjustment system. For example, the Justice Department is litigating actions against UnitedHealth Group, Elevance Health, and KaiserPermanente regarding the accuracy of their diagnosis data used for risk adjustment. In September 2023, Cigna paid $172 million dollars to the federal government in order to resolve False Claims Act allegations that it provided inaccurate data on patients’ diagnoses to inflate payments, though there was no determination of liability.
During FY 2023, efforts by the Health Care Fraud and Abuse Control Program for Medicare, Medicaid, and other government programs resulted in recoveries of $3.4 billion, of which the Medicare Trust Funds received close to $1 billion. The ROI for the HCFAC program from 2021 to 2023 is $2.80 returned for every $1.00 expended toward addressing fraud and abuse.
The GAO, which examines how taxpayer dollars are spent and provides Congress and federal agencies with information to help the government save money and work more efficiently, has undertaken a series of studies looking at these issues in the Medicare and Medicaid programs. A recent report from GAO found that while CMS has implemented numerous GAO recommendations to reduce improper payments in Medicare (as well as Medicaid), there are additional opportunities to improve program integrity in these programs and save billions of dollars. GAO also annually publishes a high-risk series that identifies government operations vulnerable to fraud, waste, and abuse, and Medicare has been on this list since 1990 due to the size and complexity of the program. In addition, in 2015, GAO established a framework to manage fraud frisk in federal programs, which CMS uses for implementing its Medicare integrity programs.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.